What is SUGAR?
The SUGAR Story & Data
In 2010, we began meeting annually with a group of pediatric global health education colleagues from seven institutions in the Midwest to share best practices and research ideas. Through this Midwest Consortium of Global Child Health Educators we realized that despite the substantial effort we were putting into preparing our residents for global health rotations, we had not yet found a way to adequately prepare our residents for the emotional challenges that they encountered abroad.
At the same time, Mike and Sabrina had been using simulation in their respective global health programs to develop a resident-led simulation curriculum with an international partner and to help residents learn about medical conditions they were unaccustomed to seeing in the U.S. As we shared our respective simulation experiences with our Midwest Consortium colleagues and reflected on the gap that all seven programs perceived in pre-travel preparation, it led us to ask the question “could we use medical simulation to prepare global health residents for common emotional challenges encountered abroad, rather than just medical preparation?” It was this pivotal moment that led to the development of the SUGAR curriculum.
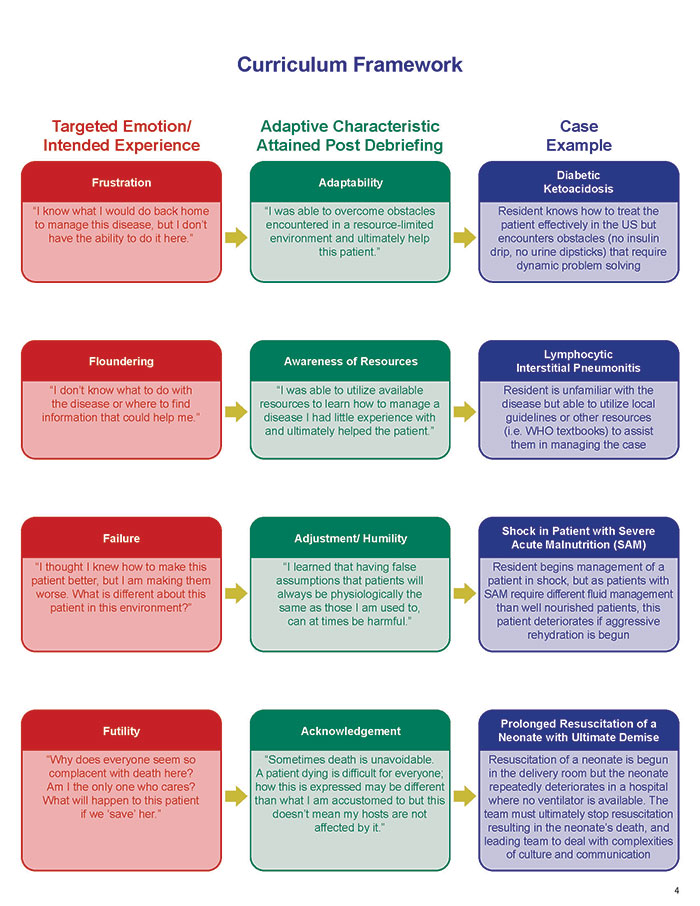
To develop the curriculum framework, we pooled our shared experience and identified themes that we consistently observed during post-travel debriefing sessions with our residents. We compared these observations with what has been reported in the literature with respect to emotional challenges faced by trainees during global health rotations abroad. We prioritized this list to include the following important emotions: frustration with the lack of resources, floundering when encountering an unfamiliar disease, dealing with failure when things didn’t go as expected, and wrestling with perceived futility, mismatched senses or urgency, and death & dying.
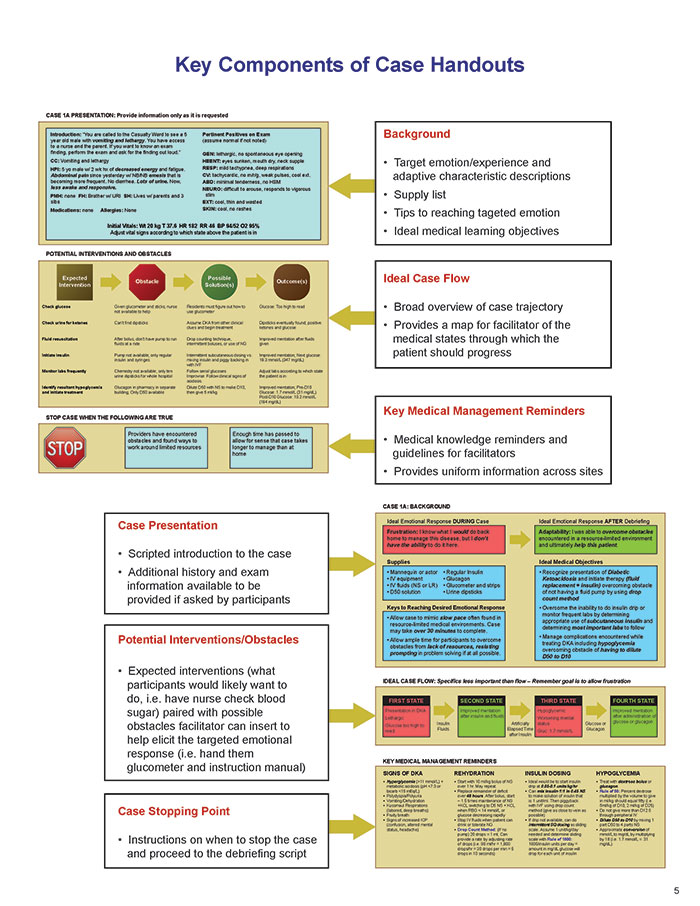
We then set to work to create simulated cases that would mimic resource-limited settings and allow residents to experience and debrief some of these challenges prior to growing abroad, rather than feeling them the first time thousands of miles away. We created eight cases that address the target emotions (“the four Fs”), which were paired with ideal adaptive characteristics that could be attained through skilled debriefing (“the four As”). We developed a streamlined case handout that includes the SUGAR paradigm; in this paradigm the facilitator focuses on introducing realistic obstacles to the learners’ expected interventions mirroring what one might encounter in a resource-limited setting.
In 2013 we piloted these cases at the seven institutions making up our Consortium and found some exciting data after 160 resident encounters:
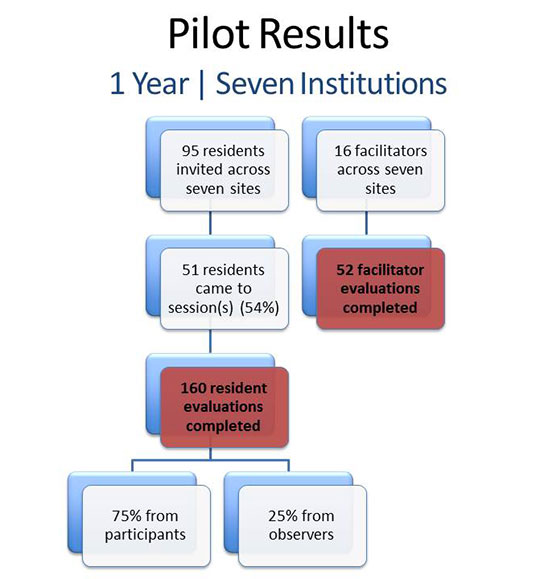
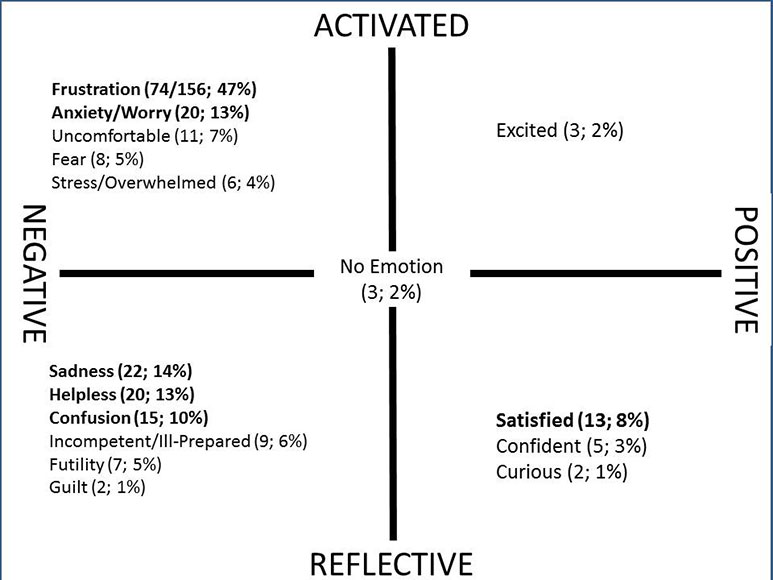
98% of residents discussed experiencing strong emotions during the case and nearly all mirrored the negative emotions encountered abroad (i.e. frustration, sadness, helplessness, unprepared, etc.)
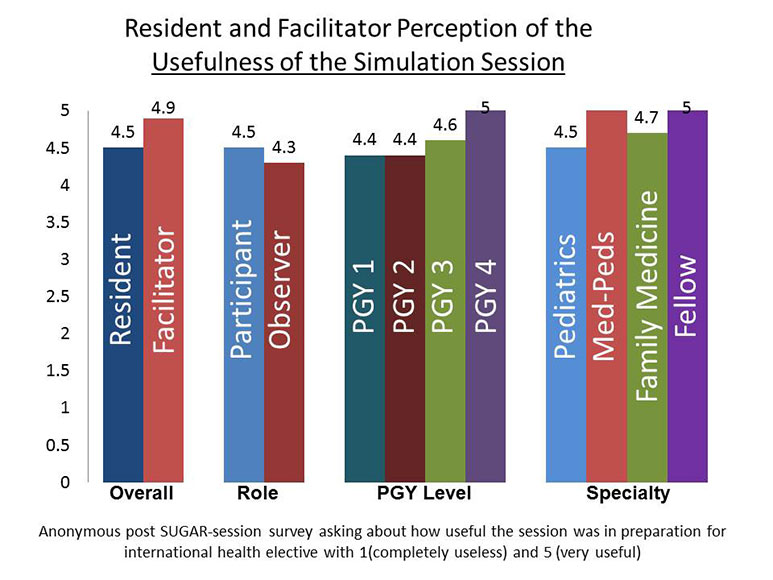
Despite these negative emotions encountered in the case, residents rated the experience as useful or very useful for preparation (4.5 on a scale of 5). Facilitators also felt the sessions were useful for preparation (4.9 on a scale of 5).
Moreover, 98% of facilitators’ comments (n=52) described the cases and debriefing script as providing the information needed to lead the cases. In addition, they felt that the cases were extremely useful in eliciting the intended emotions (4.8 on a scale of 5).
Further, 94% of residents said the SUGAR experience would change the way they would prepare before for going abroad [Butteris SM, Gladding SP, Eppich W, Hagen SA, Pitt MB, Investigators S. Simulation Use for Global Away Rotations (SUGAR): Preparing Residents for Emotional Challenges Abroad-A Multicenter Study. Academic pediatrics 2014; 14(5): 533-41.]
Based on the success of our pilot, we began leading workshops to train facilitators to implement the SUGAR curriculum at their institutions and facilitators across the country are having similar SUGAR success. We also now beginning to collect formal feedback from residents who have participated in SUGAR and have since returned from their global health elective and are finding that residents continue to find the sessions as useful in their preparation, and the themes identified as helpful appear to be similar.
Want to know more about SUGAR?
What Are SUGAR PEARLS?
PEARLS stands for Procedural Education for Adaptation to Resource Limited Settings and is a SUGAR Spin-Off Curriculum. Are you treating an infant in respiratory distress but you don't have access to a ventilator? Do you have a patient with a complicated pleural effusion but you don't have a chest tube drainage system? Providers working in resource-limited settings must routinely modify the way they perform procedures using available supplies and creative problem solving and these video PEARLS organize and disseminate some of these strategies for performing procedures in resource-limited settings.
Interested in bringing SUGAR to your institution?
Frequently Asked Questions about the logistics of implementing SUGAR
Learn what you need to know to become a facilitator